National physical culture shall be promoted. Public health and medical work shall be expanded and attention shall be paid to the protection of the health of mothers, infants and children.
With the help of League of Nations (predecessor of the UN) health reformers, the GMD government started in the 1930’s to build a nationwide network of medical institutions in urban and rural areas. Cities had priority but the healthcare was unevenly distributed. For example, in certain areas of Tianjin, tap water was readily available and residents enjoyed adequate nutrition, while in other areas, people had to resort to drinking water from stagnant ponds and faced starvation. In 1949, infectious diseases such as tuberculosis, neonatal tetanus, dysentery, and encephalitis were the leading causes of death in Tianjin, stemming from factors such as poverty, malnutrition, substandard housing, contaminated water sources, and inadequate maternal and infant healthcare. Even after the take-over, the specter of epidemics persisted. Tianjin boasted a relatively rich array of medical resources, but the challenge lay in their unequal distribution. Addressing these entrenched public health issues required substantial efforts to elevate living standards and establish a robust healthcare infrastructure, necessitating significant investments of time, funding, and personnel from the new government.
Medicine was practiced by medical missionaries and Chinese students who had studied with them in China or abroad. Both had different goals. Missionaries often utilized medicine and health campaigns strategically as opportunities to propagate their religious message and garner converts. In contrast, Chinese doctors perceived medicine as a means to contribute to the development of the emerging Chinese nation by enhancing the health of the population and imparting enlightenment through Western science.
The extraterritoriality rights granted to medical missionaries, unlike those of native doctors and Chinese health ministries, posed significant challenges in developing collaborative programs. This not only led to a division between medical missionaries and Chinese doctors but also hindered effective collaboration among missionaries themselves. Given that missionaries belonged to diverse sects originating from various Western nations, each with its own medical practices, they were separated both by ideological beliefs and professional approaches. After 1949, the medical organization was modelled after the Soviet system with its emphasis on constructing urban hospitals, industrial clinics, trade union sanatoria, and
technically advanced central medical research institutes. Similar to other sectors of society, the CCP found itself dependent on GMD personnel, particularly in the medical field. The technological and scientific elite within medicine felt secure, knowing that the Communists had little option but to integrate the existing Nationalist infrastructure of both applied and theoretical medicine. This integration excluded only a few renowned physicians who had maintained close ties with the "imperialists."
In rural areas, the majority of Chinese medicine practitioners hailed from despised landlord families, who were among the few able to afford education for their sons. This social stigma resulted in patients withholding payment from this marginalized group, further diminishing their already meagre income. Additionally, these doctors' families were unable to provide support as they had lost their previous resources. To survive, Chinese doctors resorted to raising prices above government-set levels, appropriating drugs or campaign materials for personal gain, siphoning funds from communal campaign accounts, or fleeing to resume private practice. However, government pressure and concerted efforts to eradicate private practitioners often compelled their participation. While numerous economic and political decisions in early 1950s China focused on industrial and urban development, aiming to replicate Stalin's achievements in rapid state-planned industrialization, the country's national medical policies took a different trajectory. During this period, Chinese medical policies continued the organizational experiments initiated by Chinese medical reformers and administrators in the 1930s. Consequently, the Soviet influence on Chinese medical organization appeared to have impacted only specific aspects of central and urban medical institutions. These aspects included the establishment of specialized central research institutes under the Chinese Academy of Sciences and Chinese Academy of Medicine, the development of clinics and sanatoria for urban industrial workers, and the CCP's efforts to gain political control over medical professionals by restructuring their associations, journals, teaching curricula, research institutes, and health institutions at all levels.
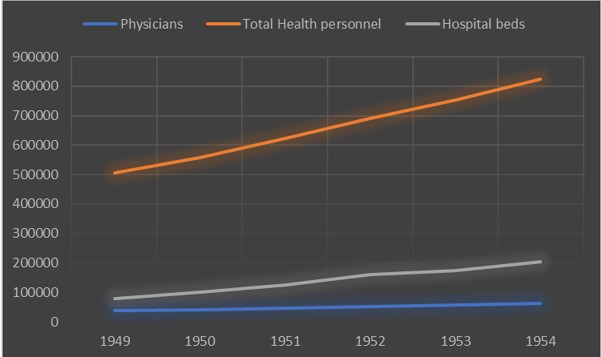
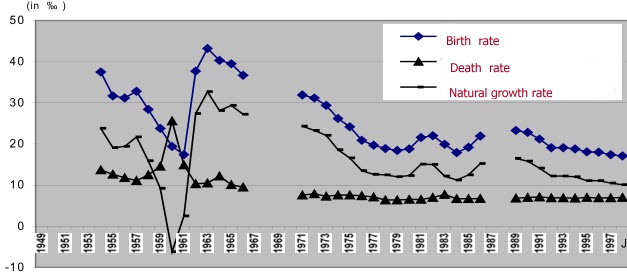
Fig. 48.1 Healthcare 1949-1954
Source: Kraus (1982). Page 331
The number of physicians at the time of the founding of the PRC fluctuated in several sources from 10.000 to 41.000.
Practical measures were frequently implemented to improve public health. Concerned about the risk of epidemics, the Military Control Committee took decisive action where the Guomindang had merely relied on propaganda. In early June 1949, over the course of just eight days, the committee directed the army to clear 38,000 tons of garbage from the streets of Shanghai.
In 1952, the national health policy can be described as priority for the needs of workers, peasants, and soldiers, prevention, unity of Chinese and Western medicine, and the combination of health work with mass movements.
In 1952, two health insurances were introduced. One, which covered all government employees, college students and staff, and employees in political parties and mass organizations. This insurance was subsidized with governmental assets devoted special to this purpose. (See Article 2 for restriction of mobility) The other one was designated for all workers employed by state-owned enterprises. This was funded with the contribution of the firms. See also Article 32 Peasants had to pay for their medical care on a fee-for-service basis. As soon as the agricultural collectivization started, cooperative health care was introduced. Yet the provision of rural medical services was below par.
In addressing the severe shortage of healthcare professionals in rural areas, a human resource development strategy was implemented in 1951, comprising three key components. Firstly, a reform in medical education shortened medical degrees to four years of college training and efforts were made to establish a three-year secondary level medical training program. Second, policies and campaigns were enacted to encourage healthcare workers in urban areas to contribute their services in rural regions, including participation in mobile medical teams. The Ministry of Health set a target to allocate at least one-third of health professionals and administrative staff to serve in rural areas. Third, a significant number of educated farmers, referred to as 'barefoot doctors,' were recruited and underwent a three-month training to provide basic primary health care services in rural areas. This initiative began in 1951, with the Chinese government calling for primary school teachers and New Democratic Youth leaders with primary health training to engage in rural health care activities without disrupting their regular work and production activities.
Fig. 48.2 Chinese Government’s Health Expenditure during 1952-1953
Source: Academic Center for Chinese Economic Practice and Thinking (2019). Page 23
GDP: Gross domestic product A fourth way to improve the health care system was a tax exemption policy, which was established in 1950, exempting all categories of health facilities from paying taxes. This policy permitted health providers to retain the revenue they generated, encouraging them to reinvest it to eliminate financial barriers to the provision of health services. The policy applied to various providers, including private, collective, or public-private health providers, as well as Chinese medical practitioners. However, this exemption was contingent on their commitment to offering medical services (including free services for the PLA), engaging in epidemic prevention, providing maternal and child health care services, and allocating a portion of inpatient and outpatient services for free. Additionally, providers were obligated to adhere to health service rates established by local health authorities. Experts validating the findings considered this policy crucial for alleviating financial shortages.
Healthcare was essentially free for all, operating under a tiered system of regulation. Urban patients were initially directed to Tier 1 hospitals/clinics, with referrals to Tier 2 and Tier 3 hospitals for more specialized care if necessary. Although this healthcare system was rudimentary and basic, with low-quality care and primitive equipment, its outcomes were remarkable. Significant improvements were observed in key health indicators, such as reduced infant mortality and increased life expectancy. Health financing was predominantly centralized, with strict budgeting and financing allocated to provincial and local hospitals. There was a strong emphasis on cost control and the provision of essential services through public hospitals. The decentralized system led to variations among provinces in terms of fiscal revenues and consequent investment in local healthcare systems. Evidence indicates that the establishment and development of health institutions were notably limited in Western China, particularly in Qinghai, Ningxia, and Xinjiang provinces. Throughout the entire period, Qinghai and Ningxia provinces failed to reach a 1 percent share of the total healthcare facilities nationwide. A comparable trend can be observed for Xinjiang and the southern region of Hainan until the 1960s, with their share remaining below 2 percent even then.
Traditional Chinese Medicine...
Mao Zedong called at the 1st National health conference (August 7-18,1950) :
“Our nation's health work teams are large. They have to concern themselves with over five hundred million people [including the] young, old and ill. This is a huge enterprise, and one that is extremely important. Thus our responsibility weighs heavily . . . At present, doctors of Western medicine are few, and [thus] the broad masses of the people, and in particular the peasants, rely on Chinese medicine to treat illness. Therefore, we must strive for the complete unification of Chinese medicine.” At the same conference, He Cheng Vice Minister of Health said
"Among health workers, as among other workers, a widespread political study and ideological rectification should be carried out in order to correct the misunderstanding that medical and pharmaceutical personnel have little to do with politics. Revolutionary humanitarianism must be promoted (among them)’ Chinese medicine has to absorb scientific theory. Western medicine needed to learn from Chinese medicine, to better approach the masses. ‘the distance between Chinese and Western medicines would day by day grow smaller, and the differences between Chinese and Western medicines would day by day disappear’, until they ‘open-heartedly and inseparably unite’"
After the conference, several measures were taken. For example, every Chinese doctor had to obtain a certificate from the Ministry of Health. The purpose of this measure was to gain control on private traditional medical care. In December 1951, the Ministry of Health started “school for further training of doctors”. The initial design of these schools, which were a bridge to the final unification of both (Western and Chinese) medical systems, was to improve the traditional treatments and skills of the Chinese doctors.
In October 1952, an exam system was introduced, the examination was largely concerned with Western medicine. Most Chinese doctors failed the exam and were no longer allowed to practice medicine. Those who passed the exam were not allowed to work in 'Western' hospitals. This resulted in an even bigger shortage of doctors and the unification completely failed.
Before 1954, the Central Committee had not issued specific directives regarding the direction of Chinese medicine's development. Mao's vague statements emphasized the importance of maintaining and nurturing Chinese medicine through the slogan "unification of Chinese and Western medicines." However, the implementation and realization of this concept of "unification" fell under the jurisdiction of the Ministry of Health, leaving the specifics of its execution unclear. A second reason for this failure was the composition of the Ministry of Health. The management of the ministry was for the most part in the hands of Western educated personnel. (Fu Lianzhang, He Cheng, Su Jingguan,
Cui Yitian, the 4 vice ministers were all Western educated and the minister
Li Dequan was not educated in medicine). They were urban and Western orientated and they only provided lip service to the CCP policy. Part of the scarce budget was spent on diseases, such as tumours and cancer, subjects that at that time in China are rather irrelevant, instead of researching diseases such as typhoid fever, cholera, malaria and smallpox.
This attitude provoked a lot of criticism and in 1953, Bai Xueguang 白学光(1913-2017 ), started an inspection tour. His rapport of March 27, 1953, contained a sharp criticism of the bureaucratic conduct of the Ministry of Health.
"Leadership is not centralized, there exists a number of unresolved treatment issues as well as tremendous wastage of resources.
There’s confusion among the many sub-departments, and many cadres are discontent within the ranks of the Ministry of Health."
In October 1953, Mao Zedong stated
"The most serious one is that [the Ministry] is short on politics, short on political work. There is too little Marxism-Leninism and socialism there. The Party must exercise overall leadership;..."
On June 1954, the decision was made to establish a research institute for traditional Chinese medicine. Lu Zhijun 鲁之俊 (1911-1999), a western educated doctor but a promoter of TCM, was appointed director. The task of the institute was to systematically organize the Chinese medicine knowledge, to compile textbooks, and to educate teachers. On December 19, 1955, the institute opened.
TCM was essential to many minority groups. Often, they had their own methods and systems for healing. Especially Mongols, Tibetans, Uygurs and Dai. The government tried to bring modern medical and health care, but these efforts were frequently frustrated due to local differences, language problems, and lack of sensitivity by Han medical personnel to the local practices.
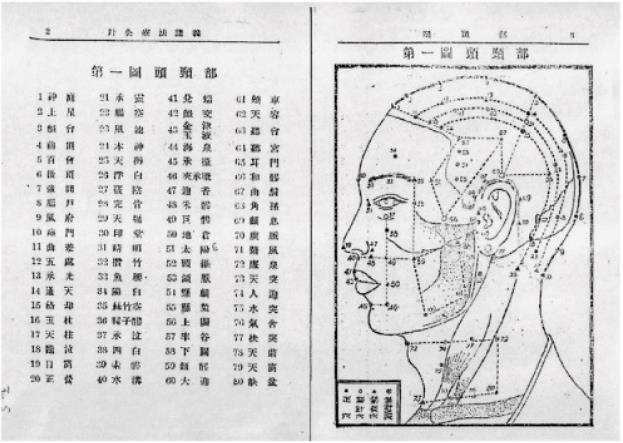
Acupuncture and Qigong...
During the Qing dynasty, acupuncture was considered ineffective. Therefore, it was no longer state-sponsored and the elite turned away from this typical Chinese medicine. From then on, acupuncture was only practiced among rural areas and lower classes. The use of herbs increased. In 1930, an acupuncture research center was founded. During the Japanese war, and the civil war the institute closed. In 1951, the school was reopened. Between 1949 and 1953, several publications were printed. At the above-mentioned school for further training of doctors, acupuncture was a minor subject. The so-called 'new acupuncture' had little effect. While science had updated the theory of disease, transformed the understanding of the body, revised manual techniques, and updated the description of individual acupuncture points, its impact on diagnostics and the selection of acupuncture points in the "new acupuncture" remained minimal. Qigong therapy is also a traditional medical practice. Previously, qigong had been used mainly in martial arts. It is the use of body, breath, and mind to cure illnesses. It was recognized by the Ministry of Health as a medical treatment, after the abandonment of so-called ‘feudal’, superstitious, or religious elements and the introduction of scientific methods. The work of Ivan Pavlov was invoked to provide a ‘modern’ and ‘scientific’ basis for qigong. In the autumn of 1953, the Ministry of Health and the Chinese Academy of Sciences organized a 35-day workshop in Beijing focusing on Pavlovian theory. Twenty-two professors, researchers, and doctors specializing in physiology, psychology, and clinical medicine participated. The workshop hailed Pavlovian theory as a pivotal and materialist approach to physiology, asserting its status as the sole theory guiding the advancement of medical science in the New China.
Health campaigns...
On February 10, 1950, the GAC announced several health regulations, the focus was on seasonal disease prevention, emphasizing vaccination as a key defense against epidemic outbreaks. The regulations detailed the proper use of vaccines for smallpox, diphtheria, and measles, and stressed the importance of regular immunization against smallpox and other diseases. It also mandated training Chinese medicine doctors in Jennerian vaccination, reflecting a broader trend of integrating different medical cultures to utilize traditional practitioners for new purposes. However, health administrators in Kunming frequently complained about the quality of these practitioners' work as vaccinators. In March 1952, Zhou Enlai was named chairman of a new central epidemic prevention committee. He specified that vaccination was to be free of charge and that, since many people might still be unaccustomed to the practice, local governments must emphasize propaganda, education, and patient “persuasion”.
China had only fifty-one thousand doctors in 1950. In most rural places, herbalists, midwives, and Chinese medicine practitioners were active. Their skills ranged from competence to quackery.
Mao Zedong mentioned an important obstacle for all health campaigns
"Agricultural production is the predominant work in the countryside. In the countryside all other types of work revolve around agricultural production and serve its interests. All so-called work assignments and work methods that may hinder the peasants from carrying out production must be avoided...nor is it possible to interfere too much with the peasants. "
Another challenge was that campaign efforts, from the provincial level down to individual villagers, were driven more by budget constraints than by what would be most effective.
Health posters
The promises made by propaganda, which stressed complete eradication of disease and the reality, with outcomes of only 60% or less cure rate, resulted in the patient’s feelings of betrayal and deception. Propaganda methods used include movies, slideshows, plays, children book and posters. See for more posters Hygiene posters
Most rural areas lacked electricity and ‘old’ techniques were used like opera, theatre, story-telling, and songs. These methods were excellent to stir emotions (land reform campaign) but insufficient to transmit scientific information. This use of traditional entertainment subverted CCP ideology of crushing superstitious beliefs and popularization of science. During the early 1950s, theatrical performances and educational presentations often coincided with religious festivals, taking place at bustling markets, fairs, and holidays. While these events reached a wide audience, they often reduced snail fever campaign education to just another attraction.
The failure to transmit scientific knowledge hindered the campaign. This was at the expense of prevention which should be primary and treatment only as a supplement. In reality, prevention was neglected in favour of treatment. Propaganda for sanitation work met a big challenge, most people saw faeces, urine, saliva, garbage, and animal manure as natural and as part of the ecosystem, so managing them seemed unnecessary and intrusive. Sanitation work was considered make-work, nonproductive labor, a waste of time. Sanitation work involved interference in the environment. This intervention can prepossess feng shui, but disruption of feng shui can bring repercussions.
Women in particular were hard to convince to be treated, they were indispensable in their household duties like cleaning, cooking, tending animals and growing vegetables , caring for children, and attending the elderly. They could and would not afford to leave their homes. Since sons were seen as their social security, a woman who refused to work around the house or bear children was considered to bring misfortune to the household and jeopardize the family’s continuation. No one wanted to squander family resources on someone like that. The treatment of men was also difficult due to their working on the land.
In the early 1950s, kindergarten teachers helped combating tuberculosis through BCG injections. See Posters
At first, parents were hesitant to vaccinate their children with the experimental drug. However, following a school lecture and assurances from administrators that hospital fees would be covered in case of adverse side effects, parents decided to vaccinate not only their kindergarteners but also their younger children.
Prevention
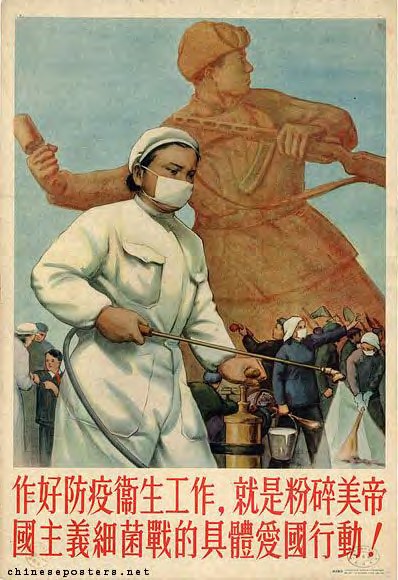
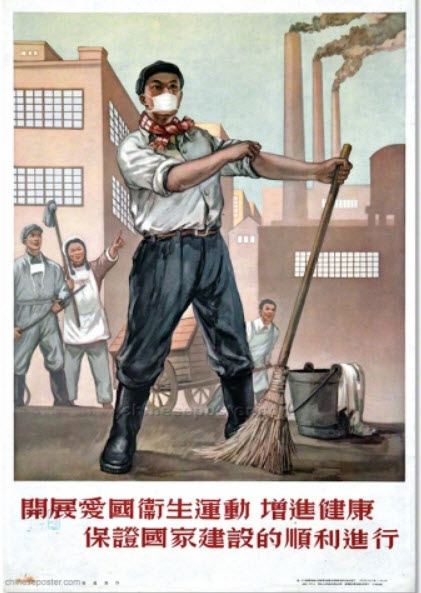
Patriotic Public Health Movement...
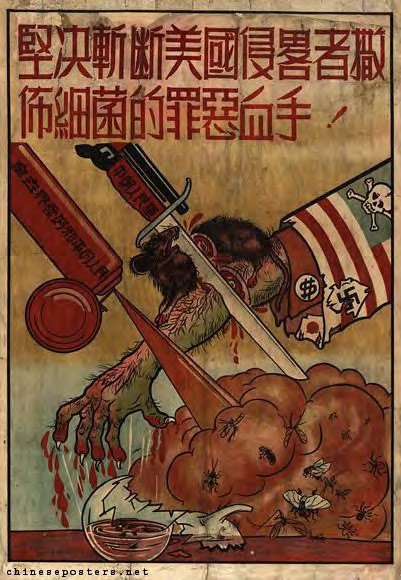
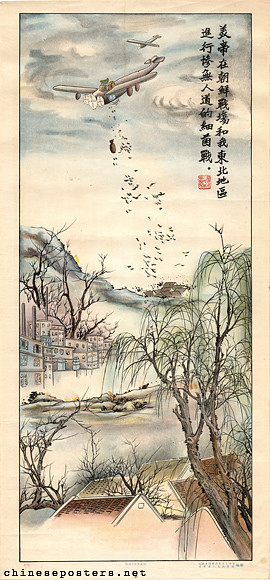
On February 23, 1952, the Renmin Ribao published for the first time about “the appalling crime of the American aggressors in Korea in using bacteriological warfare.”
This accusation was the starting signal for a national campaign called 'The Patriotic Hygiene Campaign'. The campaign emphasized that the health of the individual is just as important as the health of the state. The CCP stated that both are inextricably linked, the health of the individual is inseparable from the health of the collective.
On March 9, 1952, the CCP issued a directive:
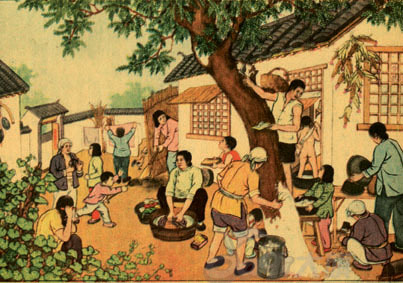
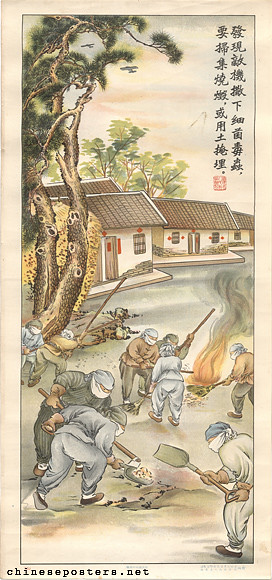
"...dividing the nation into four “prevention Regions” based on their proximity to the Korean front. It defined Korea as “epidemic Region,” the Northeast as an “emergent anti epidemic Region,” the northern, eastern, south-central, and coastal areas as “anti-epidemic supervisory Regions”, and the south-central interior, north-western, and south-western areas as “anti-epidemic preparation Regions.” Each Region was assigned with different sets of tasks. The tasks for the “epidemic Region,” for instance, included a massive program of injections, elimination of all germ-carrying animals, and designation of special hospitals for inflicted patients and quarantine of the epidemic inflicted areas." The campaign had two major goals. The annihilations of the 5 pests: flies, mosquitoes, mice and rats, lice, and bedbugs. The campaign also aimed to mobilize women and others working inside homes to participate in clearing, dredging, and sweeping the city clean. In Tianjin, hundreds of thousands of housewives, along with university and high school students, joined efforts to clear miles of the city's stagnant and foul-smelling drainage canals. Armed with picks, shovels, and shoulder-poles, residents filled in over seven hundred cesspools, one bucket of soil at a time. Neighborhood cleanups removed tons of trash from both domestic interiors and public spaces, including old derelict temples, opera halls, and street corners.
This campaign was a typical type of mass mobilization. Neighborhood committees organized meetings to convince housewives and retirees to take care of domestic hygiene. The purpose was to turn average citizens into an army of volunteer public health and sanitation workers. On the one hand, the participation level was not always high. During the mobilizations of 1952, there was significant resistance and disregard for the government's goals. While some activists from the local community participated in neighborhood domestic hygiene inspection teams, many others failed to see any connection between mundane tasks like sweeping the floor and the larger objective of defending the nation against germs. Evidently, the fear of biological weapons alone was not enough to motivate the masses to adopt modern hygiene practices.
Patriotic Hygienic Movement
Most people did not see the connection between bacteria, insects, and diseases. Diseases were only seen as a phenomenon of nature. In rural areas, the peasants noticed that the harvest had not been affected. They continued to rely on traditional practices rather than modern tools. Ironically, local religious groups, once viewed by the party as remnants of the old society, were now leveraging the movement to gain legitimacy and expand their influence, emerging as a powerful force in resisting the state's attempts to penetrate grassroots society.
According to a report from a public security bureau in Hebei, there was a common pattern observed before people began seeking holy medicine. Initially, various rumors circulated, often involving female spirit mediums and individuals claiming to be immortals visiting the earth, who actively engaged in enticing the minority of the population who were unwell to seek holy medicine. If someone with a minor illness fully recovered, rumors spread rapidly, leading the masses to believe. Subsequently, there was a significant increase in the number of people seeking this medicine.
Therefore, newspapers and radio broadcasts stopped giving only medical information but stressed germ warfare descriptions with reports about its victims.
However, there now was a rise in false alarms and exaggerated responses, indicating that fear, rather than apathy or disregard, was becoming a prevalent response. Political propaganda shifted its focus towards channelling popular fear into societal reform and national mobilization.
This campaign had two main objectives. Firstly, it aimed to engage the entire nation in the movement for disease prevention. Secondly, it sought to familiarize the populace with extensive political campaigns that impacted their daily lives. The Patriotic Hygiene Campaign served as a method for challenging the importance of medical expertise and advocating for the model of 'people's war', or mass mobilization, as the appropriate approach to building socialism in China.
Patriotic Hygienic Movement
Amid the anti-American sentiment during the Korean War, intellectuals with American training, including immunologists, were targeted. In this precarious environment, endorsing allegations of bacteriological warfare allowed Chinese immunologists to maintain political legitimacy and build intellectual authority. While some scientists lost their jobs and faced criticism in the People's Daily, others were hailed as experts serving their country faithfully. Supporting accusations of germ warfare became a political act, serving as a declaration of loyalty to the CCP and a means of avoiding persecution.
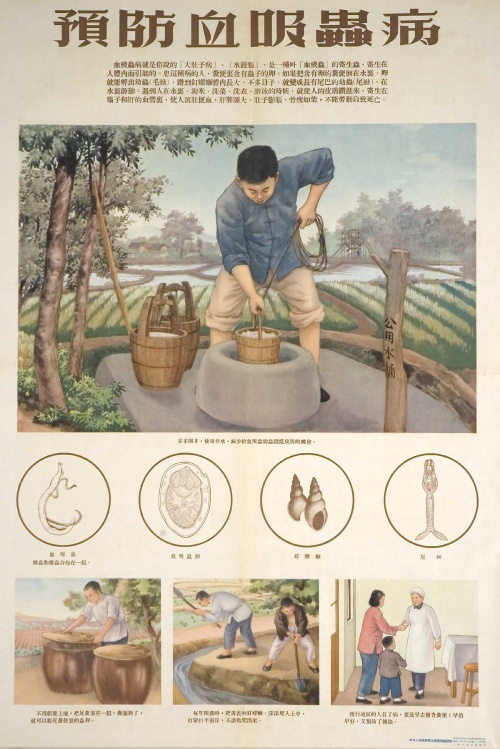
Schistosomiasis health campaign...
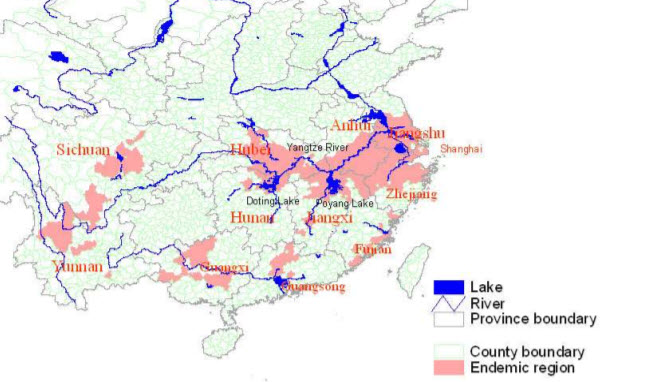
One of the most outstanding health campaigns was the schistosomiasis health campaign. The disease affected 10.6 million people, with another 100 million at risk in the southern part of China (mainly in areas along the Yangtze River and to the south of the river basin. These areas include 348 counties in 10 provinces, the Shanghai
Municipality and Guangxi Region). Schistosomiasis threatened the productivity of farmland, labor, and capital (draft animals). In the 1950s, the endemic situation of schistosomiasis was extremely serious in various endemic areas of Jiangxi province. Average infection rate for inhabitants was above 10%.
Regional distribution of schistosomiasis before the 1950s in China
Source: Guo (2003). Page 15
Due to military and economic security concerns, the new government framed the campaign as a political initiative rather than a mere health endeavor, presenting it as one of its earliest efforts to transform rural environments. Despite facing obstacles such as limited funding, scarce material resources, inadequate technical and medical expertise, and resistance from both villagers and local officials, the Party managed to achieve favourable outcomes through the campaign and established constructive relationships at the grassroots level. Examining the intricate interplay of resistance, integration, and power struggles within the nascent regime against a backdrop of resource scarcity provides insight into the campaign's complex dynamics.
See also Article 2.
The new regime could rely on personnel, infrastructure, and knowledge from the GMD administration, but it lacked resources. The CCP faced several problems in combatting the disease. Most doctors had employment in the cities and were reluctant to work in inhospitable rural areas. In the early 1950s, rural health bureaus lacked personnel to conduct a treatment campaign to promote ideas about sanitation and public health, and the power to mandate altered behaviour. The inhabitants of the newly ‘liberated’ areas had little trust in the new government.
During the Sanfan (see Article 18), local health services became disorganized, and medical workers, dissatisfied with being assigned to rural areas, used the disorder as an opportunity to return home. In some regions, the Three-Anti Campaign impacted both the quality and quantity of public health efforts for up to a year afterward.
The Chinese government viewed medicine as a convenient means to showcase the scientific underpinnings of CCP governance, aiming to lead the populace toward a modern socialist future rooted in science. This vision contrasted sharply with the perceived stagnant and superstitious past spanning millennia.
Between 1949 and 1954, the number of research papers on schistosomiasis nearly doubled over what it had been in the previous 40 years.
At the end of the 1950’s, despite all difficulties, the endemic disease was to some extent eliminated. Treatment of the disease was successful; prevention of the disease was not. True elimination occurred in most places during the late seventies and eighties.
Prevention
Anti-malaria campaign...
The goal of the 1952 anti-malaria campaign was to reduce malaria cases and lower the death rate. Several ministries collaborated to ensure its success, along with organizations like the Red Cross, ACFDW, and ACFTU. Additionally, urban communities, work units, and rural villages were mobilized. The campaign sought to transform the masses from passive recipients of medicine and health care into active participants in the fight against disease and in control of their own health. This approach became known as the "mass mobilization model" in malaria studies.
The scarcity of medicines and healthcare professionals, particularly in rural areas, posed a significant obstacle to achieving a substantial breakthrough. Posters, instead of promoting unavailable anti-malaria drugs, emphasized prevention. Such an approach partly disappointed the intended audience of the campaign and dampened their enthusiasm for health initiatives. It might have even eroded the government's credibility.
Traditional methods of moxibustion and burning mosquito repellent were promoted alongside with modern techniques of spraying insecticides. This mixed use of Western and Chinese medicine was endorsed by the government. In Yunnan, cinchona trees were cultivated to provide a reliable supply of quinine.
Anti-Drug campaign...
In December 1952, the People's Republic of China declared to be a ‘drug-free nation’. In 1949, there were estimated more than 20 million opium addicts.
From 1950 onwards, an anti-drug campaign was held. On September 12, 1950, the directive concerning the strict prohibition of opium and other narcotics. stated a strict prohibition of drug taking. Peng Zhen coordinated the campaign, many ministries (ministries of railroads, communications, interior, and public health) and organizations (postal service, customs, courts, and procuratorate) were involved.
Trade unions, mass organizations, and the CCP held large education forums and anti-drug gatherings. During these rallies, drug users were publicly shamed (and subject to detention for coercive rehabilitation) and drug traffickers were sentenced. Offenders, who turned themselves in, confessed and showed remorse, were treated leniently. Persistent offenders (e.g., drug kingpins and drug lords) were confronted with economic sanctions (fines, confiscating of property) or imprisonment or death penalty. These anti-drug campaign was mainly carried out in urban Regions and were combined with the Sanfan (see Article 18 ) and Wufan (Chapter 4 ) campaigns. Many corruption cases were related to drug trafficking. The campaign was carried out in silence, there were no newspaper reports, pamphlets, or radio bulletins. The reason for this was the accusation of the US that the PRC were still smuggling narcotics. The Chinese government assumed that the US will use news and information about drug producing and trafficking to prove its accusations. Therefore, the campaign was carried out orally. The local cadres had to mobilize the masses by holding propaganda meetings (some were especially for youth, senior citizens, women, and students). Propaganda trucks with loudspeakers broadcasted the anti-drug campaign slogans and directives. Sometimes drug offenders were placed on the circling trucks. Operas, comic dialogues, and folk dances were used to spread the campaign’s policy. During the Korea War, the anti-drug campaign was linked with patriotic behaviour and related with the “Resist Amerika Aid Korea”.
In one area, the southwest of China, the major drug-producing Region, the campaign started in 1956. The production of drugs in the southwest part of China was located in isolated and mountainous Regions occupied by minorities.
The authorities were keenly aware that in certain regions, opium remained the primary source of income for numerous households. Recognizing that attempting to suppress opium without establishing full control over these areas and without providing alternative crops would likely trigger substantial resistance, potentially leading to riots. In some areas an allowance as compensation for the lost income was paid, in some cases debtors were allowed to grow poppies until they had paid of their debts. Sometimes even compensation was paid for the loss of income for former employees of the opium traffickers.
In reality, the situation was far more intricate and diverse. Both the GMD and CCP regimes, akin to later Qing Dynasty rulers and various regional warlords, oscillated between employing severe anti-opium rhetoric and launching sporadic eradication campaigns on one hand, and clandestinely regulating and taxing domestic opium production and sales on the other. This clandestine activity served as a significant revenue source during economic downturns.
Birth control...
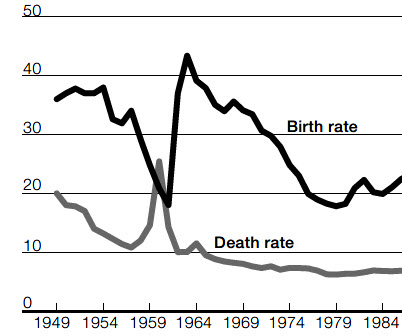
The new administration started almost immediately with health campaigns, giving information about the improvement of hygiene. The administration took measures to limit the effects of natural disasters (floods and droughts resulting in famines) by an effective central administration, improved flood control, transport, food distribution, and health services. These actions caused a lower rate of death and mortality rates and growth of the population. (The birthrate was between 1949 and 1954 annually more than 37‰. In 1949 in Guangzhou the birthrate was 27 per thousand, at the end of 1954 it had risen to 44 per thousand population)
The state embarked on the task of retraining traditional midwives and educating new midwives. The primary disparity between the GMD and the CCP in this regard was not ideological but pragmatic: the Communist Party boasted a significantly broader and more efficient rural presence, which consequently impacted a larger populace through its initiatives to modernize rural midwifery.
Fig. 48.3 Death Rates in China, 1949 to 1954
Source: Bramall (2009). Page 104
Most of the mortality reduction occurred during 1949–52 and reflected little more than the effects of the restoration of political stability. Progress thereafter was very slow.
Child mortality partly stemmed from the inadequacies of midwives. In the early 1950s, the government empowered rural women who occasionally assisted with childbirth by imparting new techniques alongside shaping their political and social roles. The Party perceived these women as practitioners with outdated methods requiring enhancement, as newly emancipated individuals necessitating a boost in political awareness, and as conventional figures in an agrarian community whose customary practices warranted regulation. Classic Chinese medical texts depicted these traditional rural midwives as uneducated, uncouth, obstinate, and hazardous.
At the end of 1951, the Ministry of Health declared that there should be at least one trained midwife per district, especially in rural areas, midwifery was quite random, the distribution was uneven, and the quality was often low. Training programs of two weeks were started for those with the right political background (oppressed and/or exploited). The two-week format emerged as the most favoured choice, as it allowed the training of a larger number of traditional rural midwives in the shortest duration, optimizing the scarce budget allotted by the provincial public health department for this initiative. On September 16, 1949, Mao Zedong spoke out about birth control:
"It is a very good thing that China has a big population. Even if China’s population multiplies many times, she is fully capable of finding a solution; the solution is production."
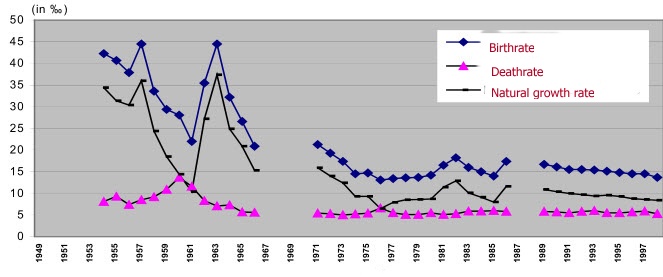
Fig. 48.4 Population development in the cities, 1949-1998
Source: Wu (2004). Page 27
Mao Zedong followed with his statement the SU, which favoured an ‘anti-Malthusian’ viewpoint. A characteristic point of view was ‘strength lies in numbers’. The People’s Daily hails the 600 million mainlanders as the most precious of all categories of capital.
A second reason for this pro-natalist opinion lies in the agriculture need for numerous children to uphold ancestor worship and to facilitate land cultivation. In contrast to the SU, a pro-natalist policy was not applied. There were no ‘Orders of the Glory of Motherhood’. However, there were likewise no institutions for birth control.
The CCP had forbidden abortion between 1931-1948 despite liberal marriage laws experiments in this period. See Article 6. A reason for this attitude was to offset the effects of disease, infant mortality, and high death rates in the base areas during the Japanese war and the civil war. At the same time, the party had encouraged young people to delay marriage and childbirth so that they could devote all their energies to the work of the revolution. In reality, the CCP maintained a two-track policy—allowing urban, educated women to practice birth control while encouraging childbearing among peasant women.
In 1952, the Ministry of Health required all entities involved in the production and sale of birth control to register with the authorities. The Shanghai government expanded on this mandate by prohibiting street vendors from selling condoms. Vendors with remaining stock were allowed to sell their existing inventory under the supervision of local health authorities, but no new supplies of condoms were permitted for sale.
Fig. 48.5 Population development in rural areas, 1949-1998
Source: Wu (2004). Page 28
In April 1950, regulations governing army and government personnel in the Beijing Region stipulated that abortion could only be carried out based on medical necessity, alongside written consent from husbands, superiors, and medical professionals. Additionally, all cadres in central government and Party organizations were required to secure personal approval from the Minister of Health.
Another factor to consider was the dominance of Western-trained medical professionals in healthcare, who, due to their traditional and conservative training, were hesitant to promote contraception. In response, the Ministry of Health enacted regulations imposing stringent limitations on access to contraception, abortion, and sterilization.
In May 1952, the Ministry of Health issued a regulation which stipulated the conditions for abortion: In cases of severe illness or threat to the woman. In addition, no woman was eligible for sterilization unless she was thirty-five years old, had six or more children, and had one child aged 10 or above. In January 1953, the import of contraceptives was banned, sparking significant frustration among women. Senior women within the party began advocating for a policy change, connecting access to birth control with the broader women's liberation movement already in progress.
Their plea was heard by the (party) leaders (in particular Deng Xiaoping, Liu Shaoqi and Shao Lizi) and in July 1954 the ban on contraceptives was lifted and the promotion of birth control started. There were no provisions for male sterilization, the argument being men could not afford to be temporarily incapacitated from surgery, so therefore women must instead bear the physical burden of sterilization.
However, the potential for this change was not solely based on this appeal of the women. Economic factors also played a significant role. By 1953, it became apparent to many Chinese leaders that the country's large population was directly exacerbating the ongoing food shortages. Although the government denied this assertion, an editorial published in April in the People's Daily asserted that the problem of food scarcity would persist due to the increasing demands of a growing population, bringing widespread public attention to the issue for the first time. In this context, Mao and other senior party leaders began to recognize the necessity of birth control measures, although these discussions took place behind closed doors.
In reality, birth control continued to be highly contentious, with medical staff generally resistant to providing information, cadres delaying necessary approvals, and contraceptives being both scarce and of low quality. As a result, abortion and sterilization remained the primary means of birth control. In essence, for many people, access to birth control was more theoretical than practical. The Chinese state's initiatives in promoting prenatal health care and introducing new birthing methods could be interpreted as encroaching upon women's social spheres, diminishing their autonomy, and reshaping societal perceptions of their gender and physiology to render them more compliant as both reproducers and contributors to the state's goals. While these campaigns undoubtedly saved countless lives and presented new opportunities for participating women, they also represented a form of bio-power. This bio-power integrated women and childbirth into a novel ideological and political framework characterized by state control, occasionally manifesting as repression.
Access to information regarding sexual health and birth control varied significantly based on demographic factors such as location, social class, and level of education. Urbanites with higher education were not only more likely to possess knowledge about birth control methods but were also among the first to access legal contraception and abortion services. While state media aimed to propagate norms regarding sexuality and reproduction aligned with national objectives, the ambiguous stance of public policy and discourse on abortion and birth control inadvertently allowed for some flexibility in individual reproductive decisions. This ambiguous landscape, consequently, facilitated diverse approaches to fertility management.
Following the Communist victory in 1949, urban sex workers and ethnic minorities emerged as the primary focal points of an anti-syphilitic campaign. The Ministry of Health orchestrated efforts to assess the epidemiological landscape of the country and develop tactics for preventing and treating sexually transmitted diseases (an estimated 10 million people). This initiative led to the establishment of a Central Research Institute of Dermatology and Venereology in 1954. Beyond medical interventions, the campaign also encompassed social and vocational rehabilitation programs for sex workers. (see Article 6)
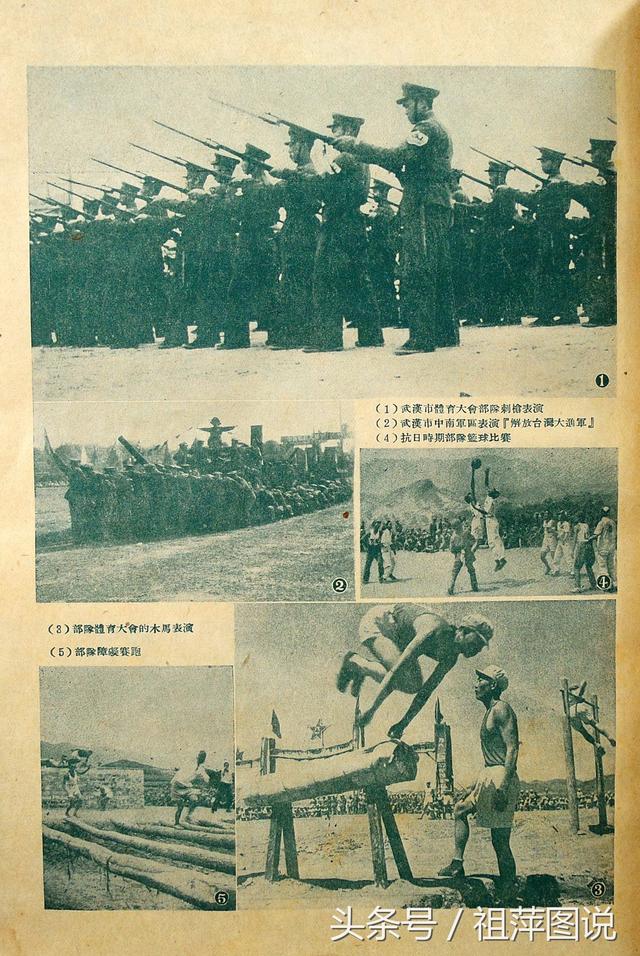
Sport...
In April 1917, Mao Zedong stated "Our nation is wanting in strength. The military spirit has not been encouraged; The physical condition of the population deteriorates daily. This is an extremely disturbing phenomenon."
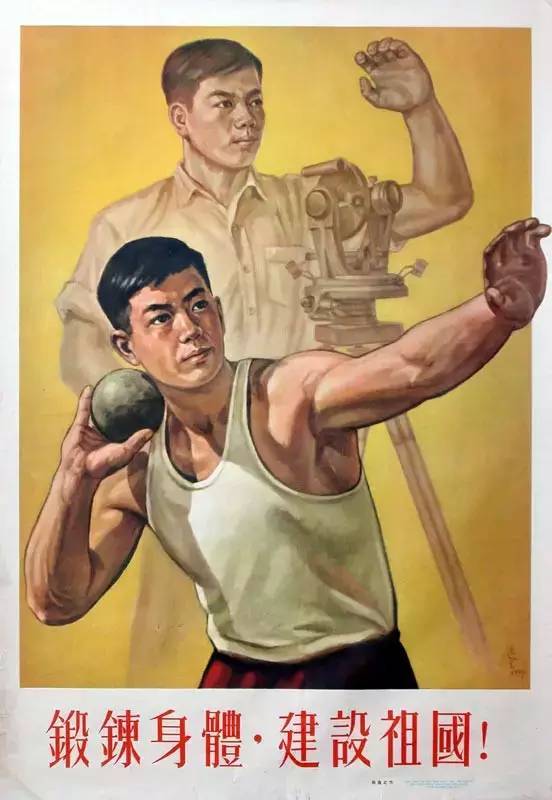
The function of sport has 3 political elements in the PRC.
1) sports serve construction, it is instrument in building a new society.
2) sports serve national defence.
3) Sports serve the people, to make sport and physical education available to the masses rather than only a privileged minority.
Physical education became a mandatory part of the education system.
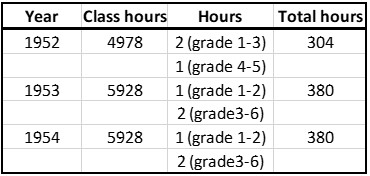
Fig. 48.6 The regulation of Physical education Hours in elementary schools from 1952-1954
Source: Jin (2021). Page 22
In the Chinese context, the term ‘Tiyu’ (体育) is often used instead of sport. 'Tiyu' also includes general fitness, traditional exercise and martial arts (e.g., taijiquan and wushu), chess, folk dance, competitive and noncompetitive paramilitary activities, collective games, and various kinds of broadcast calisthenics.
At the All-China Sport and Physical Education Congress held on 26-27 October 1949, Zhu De, vice-chairman of the Communist Party, explained:
"In the past, sport was alienated from the masses. At present, our sport must serve the people, serve national defence and serve people’s health. [. . .] In order to undertake the hard work of constructing our new country, sport should promote people’s physical and mental health. Students, workers, peasants, citizens, militants and civil servants all have to become involved in sport."
In the same year, the first national physical education convention was held in Beijing, and the State Physical Education and Sports Commission of China (SPESC) was established as the executive body to promote fitness and health. Key institutes, such as the Beijing Institute of Physical Culture, were funded by the central government with an emphasis on training athletes, coaches, physical education teachers and sports scientists (who included sports medicine in their qualifications). During the same
period, ten medical colleges offered specialized programmes in sports medicine with a focus on care and prevention of sports injuries. Six of these institutes
Beijing Physical Education University (1953), Shanghai Physical Education Institute (1952), Shenyang Physical Education Institute (1954), Wuhan Physical Education Institute (1953), Chengdu Physical Education Institute (1953) and Xian Physical Education Institute (1950) were under the direct control of the SPESC.
A policy document issued by the CCP’s CC and the Central Committee of the Communist Youth League of China declared
International sport competitions are flourishing worldwide. International friends wish China to participate in these events. Recently, we have
announced that China will send an Olympic team to the Helsinki Olympics. However, sport in China has been poorly developed in the past. After
participating in some international competitions in recent years, we are well aware of the low performance of China's competitive sports teams,
which is incompatible with China’s international status. We must change this situation! Sport must be promoted and the performance in competitive
sport must be improved19"
Only after the more or less predicted failure at the 1952 Helsinki Olympic Games (See Article 11, note 61) ,a separate ministry level sports commission
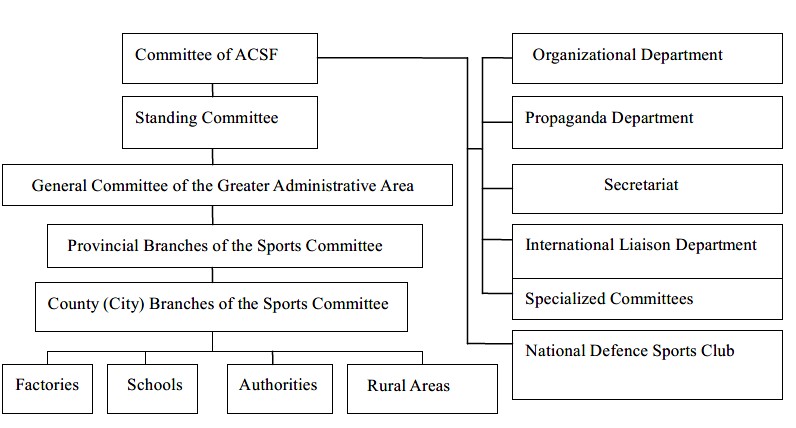
The Organisational Structure of the ACSF in 1952
Source: Shen L. (2019). Transformation of the state sports policy and system in
China (1949–1989). Page 101
was established. It had equal status to that of others, such as the Ministry of Education and the Ministry of Finance, He Long was the head. The ACSF acted as a ‘semi-state’ sports organisation, despite not being a formal government agency.
Having seen the results of the Soviet Union at the Olympic GamesRong Gaotang proposed:
"..that China should adopt the model of the Soviet Union to develop a sports policy and a centralised management system to meet the country’s political and diplomatic requirements. … The ACSF (All China Sport Federation) is only a semi-governmental organisation and it does not have the power to lead the development of sport and physical education in China. Rong argued that Chinese sport policy and practice should follow the model of the Soviet Union as it had been proved to be the most successful one in the world."
See Sport posters
Shortly after these proposals, the CCP instructed Rong Gaotang: 1) Begin the preparation of the structure of the new Ministry of Sport; 2) Begin to recruit professional full time athletes from the army and society; 3) Start to build an athletic stadium; 4) Begin to establish sports institutes; 5) Hold a National Games next year (1953).
Besides the founding of a sports commission in June 1952, also other measurements were taken, the magazine issue of Xin Tiyu in July 1950, and the start of broadcast calisthenics in late 1951. The gymnastics were broadcast by about 40 radio stations scattered across the different provinces.
A delegation observed the 1st Asian Games from 4 to 11 March 1951 in New Delhi, India. The First National Minority Nationalities Traditional Sports Games were held in Tianjin on November 8-12, 1953, with 13 nationalities and 395 athletes. Other mass tiyu activities were organized, serving as effective tools for rallying support around national and patriotic objectives that helped strengthen the new regime's power. This was especially evident during the Resist America Aid Korea campaign, which was launched after China's entry into the Korean War in October 1950. In his speech of June 30, 1953, for an audience of the Youth League, Mao Zedong explained:
"Now we must ensure that everybody is in good health; we must ensure that workers, peasants, soldiers, students, and cadres are all in good
health. Of course, being in good health doesn't necessarily mean that one will study well; studying [well] requires certain methods…. On the one hand there is study, on the other recreation, rest, and sleep; both aspects must be taken into full consideration. Young workers, young peasants, and young soldiers study as they work; for them, too, work and study [on the one hand] and recreation, rest, and sleep [on the other] must both be taken into full consideration. Both ends must be firmly grasped. Studying and work must be firmly grasped, but sleep, rest, and recreation must be firmly grasped also. In the past we only took hold of one end firmly, and we didn't take a firm hold on the other end, or else didn't take hold of it at all. Now we must develop some [programs for] recreation; there must be time and facilities [for recreation]. At this end too, we must take a firm hold. The Central Committee of the Party has already decided to reduce the number of meetings and the time [required] for study; you must supervise the implementation [of this decision]. If there are people who don't carry it out, [an explanation] should be demanded of them."
In November 1953, the authors of a report of the China National Sport Commission still complained that
"…many cadres not only did not understand the importance of sports but “have even ignored sports.”"43
Part of the reason for this complexity lies in the fact that the concept of tiyu during this transitional phase was far more nuanced than simple categorizations of “new” and “old” would suggest. It was influenced by legacies from the past, aspirations for the future, the Soviet model, and guidance from Communist revolutionaries, along with input from various experts from the pre-Communist Republican era and a few specialists from the Soviet Union. Moreover, individuals such as tiyu workers, experts, professors, and athletes who remained in mainland China after 1949 played crucial roles in shaping the trajectory of “new” tiyu, which included mentoring the next generation of athletes and leaders. Some even assumed leadership positions in national tiyu organizations. In essence, the so-called “new” tiyu of the early 1950s retained certain elements of the “old” tiyu.
In the eyes of some Party leaders the "old" tiyu experts were seen as less trustworthy than fellow cadres and thus requiring supervision.
Sport
In the 30’s and 40’s, the physical culture was based on the principles of American methods. Now, sport was considered as a weapon against American imperialism.
Feng Wenbin told
"The American imperialists spread their sport not because they were concerned about the health of the Chinese people, but because sport was an ideal tool of cultural imperialism. The American imperialists emphasised to the Chinese people that American sports equipment is the best, their athletes are the fastest and their basketball team is the top one...in the world."
Likewise, sport was seen as a weapon against feudalist martial arts. It had to be of scientific character and oppose feudal and superstitious ideas.
A notable example was the Chinese martial art of Wusu, perceived as a tool wielded by counter-revolutionary elements. These individuals established anti-revolutionary organizations that posed a threat to societal stability, imparted criminal behaviour to young individuals, and harboured enemies of the state. Consequently, the government asserted that these Wusu organizations, both in rural and urban areas, should be outlawed. Additionally, Wusu groups within educational institutions, workplaces, and government bodies were directed to undergo reorganization by the Youth League and local governmental authorities. The sport of bodybuilding had been banned because of its bourgeois vanity in 1953. Unlike mass sports, elite sports were not promoted in the early years of the PRC, as they were seen as benefiting only a select few, particularly the wealthy and the bourgeoisie. However, some elite sports were adapted to align better with the goals of mass sport development. A special kind of ‘sport’ was dancing. It was encouraged by various parties as a healthy recreational activity. However, from September 1954 onward, all dance and concert halls in Shanghai were closed, and had been changed and replaced with collective dance halls held by various units. This did not solve the problem of 'degeneration' of the youth.
Trade union organizations visited record stores to purchase jazz records, which were deemed to be "brimming with toxins." An investigation conducted by the propaganda department of the Shanghai Federation of Trade Unions uncovered instances where factory dance parties featured "yellow music" and dimmed lights, leading participants to "lower their guard." In August 1950, a sports delegation travelled to Moscow and later shared their observations upon returning to Beijing. They emphasized the importance of universal participation in exercise and recommended constructing a large stadium with a capacity of 100,000 and an indoor sports arena for 10,000 people. This advice was taken seriously; by mid-1952, the Beijing Municipal Education Bureau proposed allocating nearly 23 billion yuan to build or renovate sports facilities and provide equipment for both children and adults.
On December 20, 1950, the first Soviet Union sport delegation visited the PRC. During their stay, the delegation visited 8 cities and 14 meetings were held with Chinese officials. The development of Chinese sports programs and sports exchanges in the first half of the 1950s sought to fulfil the goals of the Common Program, while also adopting Soviet-inspired sports programs in China. PRC leaders aimed for state-sponsored sports programs to enhance the physical fitness of the Chinese populace and develop Chinese athletes to serve national objectives. Additionally, they saw Soviet-inspired sports programs as essential for advancing towards socialism and aligning with the framework of international socialism led by the Soviet Union.
Most elite athletes in the 1950s came from schools, universities and, the PLA which were the first institutional settings for women's sports.
Before 1952, the PRC did not possess a structured national team system or competition framework, aside from the national basketball team, which was the sole exception. Until 1953, most teams functioned as provisional training groups, representing the PRC in international events. For example, non-Olympic international sports events,
including competitions held during the World Festivals of Youth and Students (WFYS). For example, a delegation of eighty athletes went to the fourth WFYS in Bucharest in August 1953. Soviet and socialist bloc athletes, among the best in the world, attended these festivals.
Following 1952, aligning with the directives of "learning from Soviet Sports" and "engaging Soviet professionals in China while sending Chinese athletes to the Soviet Union," the country established national teams. Additionally, Soviet coaches and experts in elite sports were invited to introduce modern training techniques, technologies, and share their expertise.
Fig. 48.7 Numbers of athletes of national competitions 1953
Source: Dong (2004). Page 29
On February 21, 1954, Zhou Enlai delivered a speech "Building physical fitness for the motherland" in which he defined sport as a political
mission for national defence and the construction of the socialist country:
"The most urgent mission is to develop industry and the economy and consolidate national defence. This mission requires all of us to have strong bodies. We need modern technology to develop our industry. Modern technology cannot be operated without strong and healthy workers. Our people are not strong enough to be qualified workers. Furthermore, modern weapons, such as tanks and jet planes, also need strong and healthy operators. Thus, the GTO is not only designed for the improvement of an individual’s health, but also for national defence and the construction of a socialist country. It is a political mission."
The contemporary physical culture, readily embraced as "tiyu," was groundbreaking due to its systematic approach in associating "individual strength, discipline, and health" with the broader "strength" of the national body encompassing military, industrial, and diplomatic aspects. For the Chinese populace, "tiyu" not only represented sports but also served as a platform for expressing Chinese nationalism, the essence of China's national identity, and even the essence of being Chinese through public cultural activities.
Radio Gymnastics
This so-called Labour Defence System is based on the Soviet Union “Ready for Labour and Defence” system. Five fundamental aspects of Chinese physical education can be identified:
(i) The foundation was exercise, which formed the core of the physical training program. Engaging in a diverse range of exercises was regarded as preparation for all other components of physical education;
(ii) Physical education included games and dance, which were incorporated into the middle school curriculum;
(iii) Sports were viewed as an extension of basic exercises and included competitive elements;
(iv) Physical education encompassed training for labor and defense;
(v) Finally, physical education aimed to provide comprehensive patriotic and socialist education. The Labour Defence System was largely confined to schools above middle school level and the upper school physical education program, it had always a military flavour. The National Defense Sports Society (NDSS) is established in 1952. The NDSS is a section of the "Sports Ministry". Its mission was to promote parachute jumping, shooting, camping, sailing, aero modelling, radio sports, motorcycling, aerodonetics, and other military sports in the city. A total of 163 sports grounds were built around the country to serve this goal. Parachute jump towers were given the highest priority.
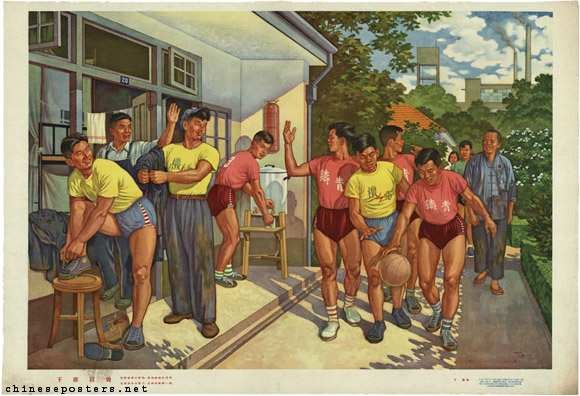
The enhancement of physical fitness was not limited to scholars and students. In 1954, a directive was issued to "Engage in Sports Activities during Breaks." Cadres in government departments at all levels were mandated to participate in ten minutes of physical exercise in the morning and afternoon on working days. That same year, the All-China Federation of Trade Unions released its "Instruction to Promote Sports in Industrial Factories" to improve workers' health.
Notes...
Duckett (1996). In Tianjin " Many of the city’s urban residents live in closely-packed, low-roofed 1950s housing that is in bad condition and often without running water or central heating. There are deaths every winter from asphyxiation because of faulty flues carrying the smoke from their coal-burning stoves." Page 140 [↩][Cite]
Gross (2010). Page 45. " She also remarks "All the doctors of whatever persuasion or nationality focused almost entirely on curative medicine, rather than preventive medicine. Preventive medicine brought in neither money, nor converts." Page 46 [↩][Cite]
Lynteris (2013). Page 16. [Cite] Rogaski (2004) however, remarks ". In preparation for making the hospitals part of the state-owned public health network, the CCP sent cadres to take inventories of all the equipment and staff of each hospital. The Communists then secretly cultivated informants within the hospitals to collect information on any anti-CCP comments or appearance of any qin Mei (close with America) attitudes among hospital staff. 15 Communists were particularly suspicious of the political sentiments of Chinese physicians who had worked with foreigners." Page 292 [↩][Cite]
Gross (2016). Page 92 [Cite][↩] See Fang (2019) for description medical care in rural areas [Cite]
Liu (2019). "...various attempts were made to avoid the abstraction “westernization of Chinese medicine” and guarantee that the transformation was under a framework of “science” but not “Western.”" Page 14 [↩][Cite]
Coussens (2008/9). Page 26. Traditional Chinese doctors, each had their own (often secret) methods and had seldom contact with each other. [↩][Cite]
Schneider (2021). Page 7 "Tier 3 and are considered to have the highest quality of care that China offers. They perform the most advanced, complex procedures and many of China’s top doctors work in those facilities3. Tier 2 hospitals are medium- sized city or county hospitals. Tier 1 hospitals are local township hospitals." Page 1 [↩][Cite]
Coussens (2008/9). Page 27. [Cite] "The term “science” was used in opposition to feudalism and superstition, which is very different from the definition in Western contexts. In addition, various attempts were made to avoid the abstraction “westernization of Chinese medicine” and guarantee that the transformation was under a framework of “science” but not “Western.”" Liu (2019). Page 14 [↩][Cite]
Coussens (2008/9). Page 33 Mao Zedong reacts on April 3: "This report of Comrade Bai Xueguang has fundamentally exposed the extremely serious bureaucratism committed by the leadership of the military’s health departments. According to Bai Xueguang’s report, the military’s health department has absolutely no leadership over the national army’s health work. This is completely unacceptable and steps must immediately be taken to resolve this issue… A department without leadership, without politics, and also not conscientiously carrying out its business - it is solely a bureaucratic department that eats, acts as an official, acts as lord and master. With the exception of the military’s department of health, there are probably also other departments equally culpable. In the current struggle against bureaucratism, please tear away the masks, bring about their total collapse, change their appearance and establish in their place organs that are truly capable of achieving some work." Page 33 [Cite] 03-04-1953 Instruction on Leadership Work of Health Departments of Military Commissions[↩]
Taylor (2005). “Henceforth the most important thing is to ask practitioners of Western medicine to study Chinese medicine, and not for practitioners of Chinese medicine to study Western medicine. Firstly, we must transfer one to two hundred graduates of medical institutes or colleges, handing them over to some well-known doctors of Chinese medicine so that they can study their clinical experience. Furthermore, they should assume an attitude of great modesty in their studies. The study of Chinese medicine by practitioners of Western medicine is honourable. This is because through the studying and improving of Chinese medicine, the demarcation lines between Chinese and Western medicine can be discarded, to form one Unified Medicine of China, as a contribution to the whole world.” Page 72 [↩][Cite]
Otehode (2016). "...some doctors of traditional medicine promoted a novel view of qigong therapy that conformed to the ideology of the new state, maintaining that ‘qigong therapy was born from the knowledge of the great working people but, unfortunately, was exploited by Buddhism and Daoism and cloaked in superstition and mystery’.35 Others simply obscured any religious connection by asserting that the origin of qigong could no longer be ascertained.36 In this way, qigong therapy was recognised by the state as part of traditional medicine." Page 78 [↩][Cite]
Brazelton (2019). Page 125 [Cite] To combat widespread infectious diseases, the government provided free prophylactic vaccines, notably against smallpox, diphtheria, and tuberculosis. Smallpox, with its high mortality rate and frequent outbreaks, was a major concern. Following the 1950 "Interim Measures for Vaccination," over 500 million people were vaccinated against smallpox between 1949 and 1952. The annual distribution of over 100 million free smallpox vaccines significantly reduced infection rates. Research team (2019). Page 24 [↩][Cite]
Fang (2008). "...herbalists, bone-setters, snakedoctors, and those villagers who used folk methods to cure common illnesses, such as tumefaction, heat stroke, and stomach bulging. Usually, these practices were family traditions that had been passed down from previous generations, 9 and the people who practiced them were not considered medical professionals by their fellow villagers....In addition to folk healers, religious and supernatural healers were very popular." Page 223 [↩][Cite]
Gross (2016). Page 79. She also mentions "The most blatant manipulation of labor and money was reserved for the prevention campaign. For snail elimination teams, in addition to withholding labor or calling people back after only a couple of days’ work, cadres often selected people with half labor power, such as the elderly; teenagers with a poor work record; and landlords, intellectuals, and others deemed bad or from reactionary political categories... " Page 85 [↩][Cite]
Landsberger (2010). "However, posters never played anything but a supportive role and merely amplified visually what was conveyed through printed or broadcast media, through mass meetings and communal reading groups." Page 6 [↩][Cite]
The anti-syphilis campaign is the first mass campaign. Syphilis is widely spread (tens of millions) particularly in minority Regions (10% of the total). At the end of the era, syphilis is under control [↩]
claims to use energy forces to harmonize individuals with their surrounding environment. Flower (2004) observes "In the fengshui idiom, roads are like rivers, liminal places where movements of energy are strong. Roads are in the abstract neutral conduits, carrying both beneficial and malevolent flows. The straighter the road, however, the more conducive it is too bad energy flows. Properly constructed roads conform to the landscape and maximize the beneficial flow in and out of the physical village; bad roads that violate the landscape cause outflows of wealth and allow malicious forces in. In fengshui logic, situations along smaller veins tapping the energy of main arteries are best; to be too near main arteries is dangerous and unlucky (...). Villagers see roads as potentially beneficial, but they also perceive roads as sources of social instability and fields of violence." Page 676 [↩][Cite]
Rogaski (2004). Page 297. [Cite] Yang (2004) writes "In designing the process, women were specially targeted because they had more free time and could play an active role in informal community activities. In the Northeast, the anti germ-warfare movement initially organized women into special quarantine groups, which later expanded to include the elderly and children. 55 In a summary of its prevention work the municipal government of Shengyang, credited its success to women activists in various residential districts who organized into an "important force in the anti-epidemic work." 56 The party's newspaper lost no time to publicize stories of women 'health stars.'" Page 174 [↩][Cite]
Smith (2006b). Page 1001. Those visitors include members of the CCP and communist youth league members. Page 1009.[Cite] Often local cadres compromise with the local people because the fight against superstition has a low priority in comparison with grain requisition. "In one county in Yunnan province, the new market was unsuccessful because officials had located it in a place said by the locals to be frequented by ghosts.49" Li (2019). Pages 241-242 [↩][Cite]
Gross (2010). Pages xvi-xvii. [Cite] Fan (2008) claims"More importantly, it was obvious that Mao, the Communist Party, and the central government had little interest in schistosomiasis prevention programs. Without their support, local governments could do very little. Although the disease was recognized as one of the most serious in eastern China in 1951 (Li 1958; Section of Health 1951), it was not listed as one of the “serious diseases harmful to people” in the government’s first five-year plan in 1953. The leaders of the central government did not appreciate the gravity of the disease, and Mao and the Ministry of Health never treated it as a national public health issue." Page 178 [↩][Cite]
Gross (2010). Page 478. [Cite] See also Zhou (2020). Pages 17-71 [↩][Cite]
Berry-Cabán (2007) notices "Some of this research was of the standard fare: testing various molluscicides, from copper sulfate to Paris green and DDT; testing various antimony drugs for their therapeutic effects; surveying reservoir hosts; and searching for more reliable diagnostic methods.
However, other aspects of this research such as finding methods of killing schistosome eggs in feces stored for fertilizers and testing native herbal drugs for their therapeutic and molluscicidal effects had a uniquely Chinese flavour." Page 48
[↩][Cite]
Shen (2017). Oddly in 1953 the Hekou farm (a technological innovation place) was "...transformed into a new experimental field for rubber plantations to supply “communist” rubber to the Soviet Union." Page 229 [↩][Cite]
Biddulph (2007). "On 18 December (1952) the CCPCC issued Luo Ruiqing’s ‘Concluding Report on the Nationwide Campaign to Eradicate Drugs’, marking an end to the campaign. During the campaign, police commentators assert that 345,463 drug users were registered, 82,056 people were arrested, 880 were executed and the balance punished with life imprisonment, fixed-term imprisonment, reform through labour or control, with a small number released" Page 80 [↩][Cite]
Lu(2016). "During the initial phase of drug prohibition under the PRC, several major national and Regional laws and decrees were issued. These included the 1949 Temporary Measures on Prohibiting Opium and Other Narcotic Drugs in the Hubei Region, the 1949 Temporary Measures on Prohibiting Opium Smoking in Suiyuan Province. The 1950 Decree on Banning Opium issued by the Executive Administrative Ministry, the 1950 Measures on Completely Eradicating Opium issued by the Southwestern Military Government Committee, the 1951 Measures of Eradicating Opium Smoking in the Inner Mongolia Autonomous Region, and the 1952 Directive on Prohibiting Opium and Other Narcotic Drugs issued by the Northeastern People’s Government. Page 89. [Cite] 24-02-1950 GAC directive concerning the strict prohibition of opium and other narcotics. 19-04-1951 The Ministry of Internal Affairs Reports to Zhou Enlai on the 1950 Opium and Drug Prohibition Work [↩]
Zhou (1999). Page 161 In the southwestern province of Yunnan, where one-fifth of the agricultural areas were occupied
by opium poppy cultivation, a quarter of the entire population of the province; entire villages, including women and children, smoked opium.
[↩][Cite]
Fang (2007). Page 6 [Cite] Li (2014). After April 1950, the survey and registration of old midwives was carried out in the entire East China region, and a total of 11,636 old midwives were distributed in towns and villages in Shanghai, Nanjing, northern Jiangsu, Shandong, Fujian and other places. From 1950 to the first half of 1951, health institutions in provinces, cities, and counties in the Northeast, together with relevant departments such as the Women's Federation, carried out large-scale registration and training of former midwives. A total of more than 30,000 former midwives were registered. the Ministry of Health held the first national maternal and child health work symposium in Beijing from August 17 to 22, 1950. The meeting put forward the working principle of "reforming the old midwives and promoting new delivery methods". According to statistics from the Ministry of Health, in 1950 alone 91,224 former midwives were rehabilitated. No page number [↩][Cite]
"Six Hundred Million People - A Great Strength for Socialist Construction of Our Country." RMRB 01-11-1954 [↩]
"An ancient Chinese peasant proverb says: If you are planning for one year, sow grain; if you are planning for ten years, plant trees; but when you are planning for a hundred years, grow men." [↩]
Liu Shaoqi states "Should China praise "heroic mothers" and encourage more births?
No. We should not, and I don't think we should do it in future either; probably we can never do so.", but there are likewise no institution for birth control." 27-12 1954 Liu Shaoqi Encourage birth control [↩]
Jeffreys (2004). Page 1017 [Cite] Dikötter (1993) Page 344.[Cite] Chen (2020). Syphilis and other sexually transmitted infections (STDs) were major public health and medical concern in early time of the foundation of New China in 1949. According to the data gathered during that time, the prevalence of syphilis was as high as 84.9% among women who sold sex in Beijing,6 5%–10% of the population in some urban communities and 0.5%–4% of rural residents in some areas.7 In 1949, syphilis accounted for about one-tenth of patients in the dermatology department of the Beijing Medical College.8 Syphilis was also a serious health problem in some minority areas due to local customs. In a study in minority areas of five provinces (including Inner Mongolia, Xinjiang, Yunnan, Guangxi, and Gansu), syphilis prevalence was found to be 57.2% in 1951 and 44.3% in 1952. By 1950, it was believed that there were more than 10 million persons infected with an STD, most of them suffering from syphilis in China.9 Page 193 [↩][Cite]
Shuman (2014). Page 4. Broadcast calisthenics are sets of exercises broadcast on loudspeakers and designed for ordinary people to perform on a routine basis. Page 72 [↩][Cite]
The Shanghai Institute of Physical Education was established in 1952 by merging the physical education departments of Nanjing University, the East China Normal University and Jinling College. The Beijing University of Physical Education (BUPE) is the country’s major institution of physical education. Of the six institutes of physical education which operate under the jurisdiction of the Department of Sports Science and Physical Education of the All-China Sports Federation, only the BUPE recruits nationwide; the other five institutes recruit athletes and students on a regional basis. The Wuhan Institute of Physical Education serves the provinces of Hebei, Henan, Hunan, Guangdong and Guanxi. The Shenyang Institute of Physical Education recruits athletes and students from Heilongjiang, Jilin, Liaoning
and Mongolia. [↩]
Fan (2010). Page 2383. 1st National Games is only being held in Beijing in 1959
[↩][Cite]
Lu (2011). "25 to 50 percent of each monthly issue in the early 1950s to topics such as the structure of the Soviet system, Soviet tiyu theory, Soviet training methods, and successful Soviet athletes. "Targeting cadres and teachers in "physical education, athletes, and sports enthusiasts in the army, factories, and schools, this magazine published news stories about sporting events in the PRC, featured photographs of folk exercises, introduced athletics in other communist countries, and set up such columns as “exchange of pedagogies of physical education,” “short stories,” and “science of exercise and physiology.”" Page 179
[↩][Cite]
Fan (2010). "The Asian Games started in 1951 under the leadership of the Asian Games Federation, which was recognized by the IOC. The games took place every four years. Taiwan was a member of the federation and participated in the Asian Games three times between 1951 and 1958. The PRC was excluded." Page 327 [↩][Cite]
Shuman (2014). Page 68 [Cite] In 1952, the CMC decided to hold the first All-Army Sports Games in Beijing. This military sports event was also the first comprehensive sports event in the country since the founding of New China. More than 1,800 athletes participated in the sports meeting, coming from all major military regions and branches of the military. In 1953, the CMC decided to establish a military sports school in Guangzhou specifically to train sports cadres. It was responsible for the training of military sports teachers, sports directors.[↩]
11-04-1951 - 23-04-1951 Ministry of Health convened a national professional conference on epidemic prevention, and formulated a prevention and control plan for 19 infectious diseases such as plague, cholera, and smallpox
15-03-1951 Provisional regulations governing the management of hospitals and clinics.
18-02-1952 Nie Rongzhen reports to Zhou and Mao on biological warfare
08-03-1952 Zhou makes a statement protesting the US use of bacteriological weapons
14-03-1952 GAC establishes in Beijing the Central Committee of Diseases Prevention
07-04-1952 Chinese investigating commission on biological warfare in Korea reports
15-04-1952 CC “Directive on Eradication of Drug Epidemic”
15-04-1952 CC disease prevention campaign is to improve public health
20-06-1952 the All-China Federation of Physical Culture is established
27-06-1952 Free medical care for workers in government and noncommercial organizations
18-12-1952 End of the campaign to eradicate drugs
03-04-1953 Mao "Instruction on Leadership Work of Health Departments of Military Commissions"
04-06-1954 Mao decides to set up a Research Academy of TCM
December 1954 Meeting of the St. Com. CC traditional Chinese medicine